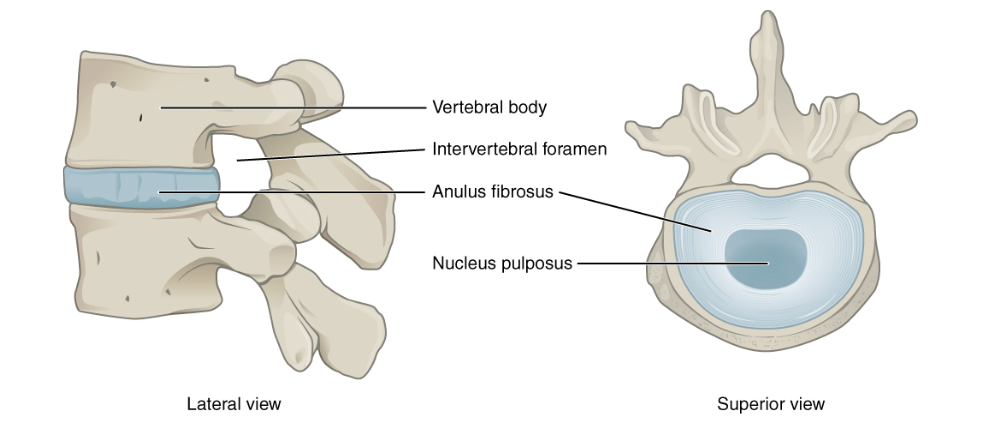
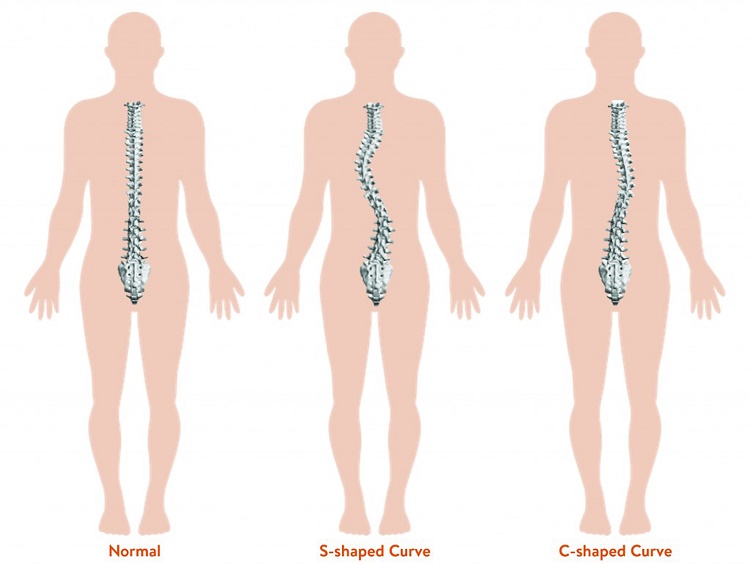
The spine is made up of vertebrae that stack up one on top of the other separated by discs. Looking from behind the spine usually stacks up with one vertebrae straight on top of the one beneath. In scoliosis however the spine is deviated from the midline creating a ‘C’ or ‘S’ shape curve. This deviation from the midline is a combination of the vertebrae curving to the side coupled with rotation.
Scoliosis can vary from a mild curve causing little or no symptoms to a severe curve, which may require treatment. Treatment is most effective when the scoliosis is detected early and managed with appropriate strategies based on the degree of curve.
There are several different types of scoliosis
- Congenital
- Neuromuscular
- Idiopathic – this is the most common form and is classified according to when onset was identified – infantile, juvenile, adolescent or adult. The most common type is adolescent idiopathic scoliosis (AIS). We will further discuss AIS in this blog.
Adolescent Idiopathic Scoliosis (AIS)
- Girls are affected 8-10 times more than boys
- Only 3 in 1000 girls will require further treatment
- There is often no pain or other symptoms at the time of diagnosis
- The exact cause of AIS remains unknown but it is important to note it is NOT caused by “bad posture”, a soft mattress, watching too much TV or carrying a heavy school bag, although these things may exacerbate symptoms.
- The most significant risk factor for developing AIS is a family history of the condition.
It is important to screen for AIS at key ages. The Spine Society of Australia recommends screening at 10 and 12 years of age as this is the usual age for the largest growth spurt and the first signs of scoliosis.
A fact sheet is routinely distributed to girls in school with information for home screening. You can find this fact sheet here.
Signs of Scoliosis
- Uneven shoulder heights
- Uneven shoulder blades or one shoulder blade that seems more prominent
- Uneven hips or one hip that seems more prominent
- More of a gap between the arm and waist on one side
- An obvious curve in the spine
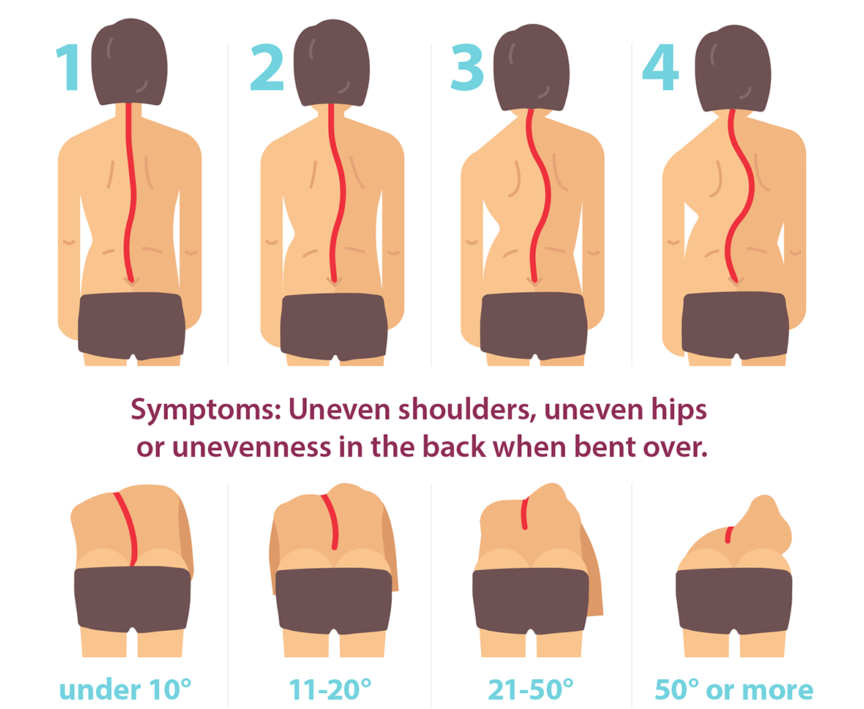
Image supplied by National Scoliosis Centre
The curve of the scoliosis can be classified according to how mobile it is:
Structural scoliosis is a fixed curve in the spine and the most common form in Adolescent Idiopathic Scoliosis (AIS). A structural curve usually has a physical structural change in the vertebrae.
Functional scoliosis is not structurally fixed. That is, the curve will bend with movement and may straighten again. It can be caused by:
– muscle spasm as a result of injury or compensation for a structural scoliosis curve
– overuse of the muscles on one side of the spine due to sport or occupation
– a difference in leg lengths
A note on scoliosis in adults:
– scoliosis may be first diagnosed in adulthood if a previously undiagnosed AIS curve has progressed.
– scoliosis may also develop in adulthood secondary to degenerative changes in the spine such as osteoarthritis and degenerative disc disease.
How Osteopathy can assist
Treatment for scoliosis varies depending on the type and severity of the curve.
Our osteopaths will perform a complete assessment, including specific scoliosis screening tests, determine a diagnosis of your pain and refer you if an x-ray or specialist assessment is required.
Osteopathic techniques including joint articulation/mobilisation and soft tissue release may help to improve spinal mobility, reduce back muscle tension and decrease pain.
Exercise, strengthening and stretching are important parts of maintaining spine health and our osteopaths can chat to you about some options and tailor a program to you.
If we assess the scoliosis to be severe and requiring different treatment such as bracing, our Osteopaths can refer you to the appropriate health professionals.
If you would like your spine assessed or your child’s screened for Scoliosis, contact us or make a booking here